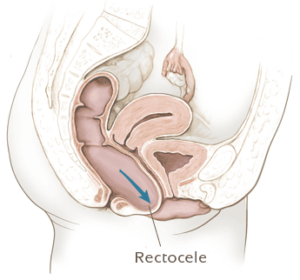
Rectocele treatment
Treatment is only necessary when the rectocele’s symptoms have a negative effect on the patient’s daily functioning.
There are several medical and surgical options for treatment. The severity of the rectocele determines the doctor’s choice of treatment.
Preventing and reducing complaints
Initial treatment includes dietary measures and physio-therapy. To prevent constipation and excessive pushing, the patient must have a regular bowel pattern. A high-fiber diet (25-30 grams per day) and a daily fluid-intake of at least 6 glasses are recommended.
Additionally, pelvic floor exercises or laxatives may be recommended. Sometimes local pressure to the posterior vaginal wall can help defecation.
Surgery
For correcting a rectocele, several surgical procedures with minimal morbidity exist. The most appropriate type of surgery depends on the size of the defect and the associated symptoms. Therefore, a successful surgical rectocele procedure requires a multi-disciplinary and specialized team.
Depending on the point of access, the procedure is trans-anal, trans-vaginal or trans-abdominal.
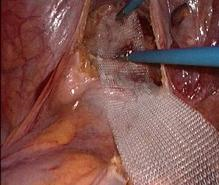
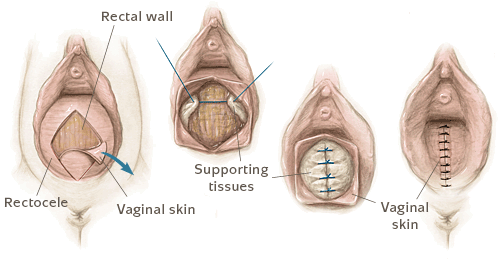
- Trans-vaginal reconstruction is carried out by suturing (plication) of the recto-vaginal septum, either with or without a synthetical mesh for reinforcement. Even though this procedure causes more blood loss and requires more pain medication, it tends to yield better results than a trans-anal procedure.
- Trans-anal reconstruction is mostly recommended when the patient has considerable difficulty expelling stool and in case of rectal prolapse (intussusception). The excess tissue is removed using a circular stapler.
- Finally, doctors may opt to perform a trans-abdominal procedure, openly or laparoscopically. In both cases, the recto-vaginal septum is completely dissected, and the front rectal wall is reinforced with a mesh. Next, the surgeon fixates the rectum to the tailbone (ventral rectopexy). This procedure is also an option when constipation and prolapse coexist. Furthermore, trans-abdominal repair is recommended when there are other pelvic floor defects as well.

Possible complications include bleeding, mesh infection and relapse.